Immediate and early hospital management of meningitis
Early hospital management of suspected bacterial meningitis in adults and children is summarised in Management of suspected bacterial meningitis in adults and children.
As soon as a patient with suspected bacterial meningitis arrives in hospital, collect blood samples for culture, and swabs or aspirates of punctured skin lesions (for Neisseria meningitidis). It is not necessary to collect additional samples if samples were collected before arrival at hospital. Perform a lumbar puncture as soon as possible, unless contraindicated, because cerebrospinal fluid (CSF) microscopy and culture is key to diagnosis. It also allows directed antibiotic therapy. For advice on CSF analysis, see CSF analysis in patients with suspected meningitis.
The timing of antibiotic therapy depends on whether a lumbar puncture can be promptly performed; see Antibiotic timing in patients with suspected bacterial meningitis. Ideally, antibiotics are started after investigations have been performed and within 1 hour of presentation to hospital.
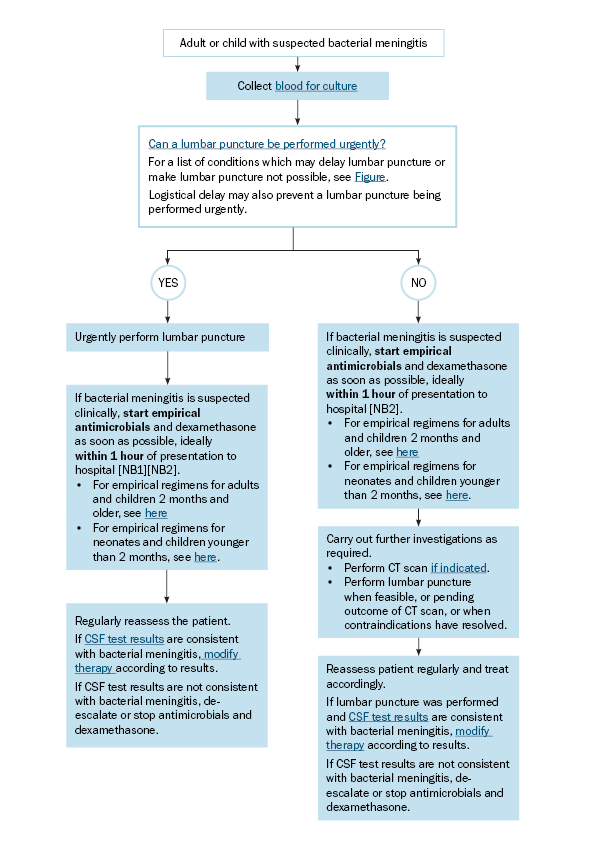
CSF = cerebrospinal fluid; CT = computed tomography
NB1: If clinical suspicion of bacterial meningitis is high, do not delay therapy while waiting for CSF test results.
NB2: When available, give dexamethasone before or within 20 minutes of antibiotic therapy unless the pathogen is known to be Neisseria meningitidis or Streptococcus agalactiae (group B streptococcus).