Neonatal herpes simplex infection
In neonates, infection with herpes simplex virus (HSV) can present with isolated skin or mucous membrane lesions, encephalitis, pneumonitis or disseminated infection. Management is complex and expert advice is required. If expert advice is not available immediately, see Initial management of neonates suspected to have, or born to mothers with, herpes simplex virus (HSV) infection for initial management of neonates suspected to have or who are at risk of acquiring herpes simplex virus infection.
If treatment for neonatal herpes simplex infection is required, use:
aciclovir 20 mg/kg intravenously, 8-hourly. neonatal herpes simplex infection aciclovir
The duration of treatment depends on the clinical presentation. Disease affecting the skin, eyes and mouth requires 14 days of intravenous therapy. At least 21 days of intravenous therapy is required for neonates with disseminated disease or encephalitis. Treatment for encephalitis should continue until herpes simplex virus is no longer detected in the cerebrospinal fluid—seek expert advice.
The role and duration of therapy in high-risk asymptomatic neonates has not been fully established. The risk to the neonate is related to whether the mother’s herpes simplex virus infection is primary and within 6 to 10 weeks of delivery (higher risk) or recurrent (much lower risk). Examples of higher-risk asymptomatic neonates include:
- neonates with negative herpes simplex virus polymerase chain reaction (PCR) tests, but who are born either via vaginal tract or caesarean section to mothers with primary herpes simplex virus active genital lesions at the time of delivery
- neonates with positive herpes simplex virus PCR swabs (from the conjunctiva, mouth and nasopharynx, or rectum) who are born to mothers with a history of recurrent herpes simplex virus infection.
Some experts recommend 10 days of antiviral therapy (as above) for these infants.
Oral aciclovir should not be used for initial treatment of herpes simplex virus infection in neonates. However, there is evidence for oral suppressive therapy (after completion of the intravenous treatment course) to prevent neurological recurrence following encephalitis in neonates. Suppressive therapy with oral aciclovir can also be considered in preterm neonates (to prevent early reactivation of disease) and in term neonates who have skin, eye or mouth lesions (to prevent cutaneous recurrence). Suppressive therapy is usually continued for at least 6 months. Seek expert advice.
After successful treatment, monitor all infants closely for recurrence of herpes simplex virus infection. If recurrence occurs, seek expert advice.
For more comprehensive information, see the Australasian Society for Infectious Diseases (ASID) guidelines Management of Perinatal Infections.
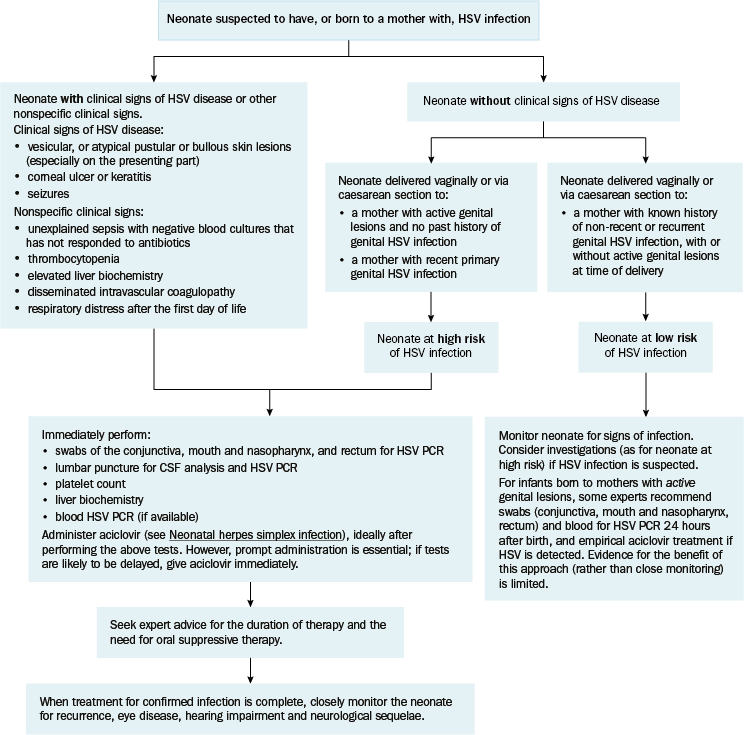
CSF = cerebrospinal fluid; HSV = herpes simplex virus; PCR = polymerase chain reaction
Adapted with permission from Palasanthiran P, Starr M, Jones C, Giles M, editors. Management of perinatal infection. Sydney: Australasian Society for Infectious Diseases; 2014. [URL]