Short stature in children
Short stature in children is rarely pathological; it is typically related to constitutional delay of growth and maturation (particularly in boys), or familial short stature. Pathological endocrine causes of short stature (eg growth hormone deficiency, hypothyroidism, Cushing syndrome) only account for about 10 to 15% of cases.
[NB1] [NB2]
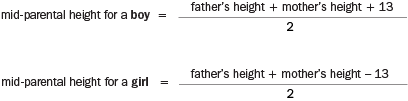
NB1: All heights measured in centimetres.
NB2: Mid-parental height may be less accurate if parents are at opposite extremes of height.
Blood tests are not required unless the child is significantly short for their family or is growing slowly. Random growth hormone measurements are not useful given the pulsatile nature of growth hormone secretion. Plasma insulin-like growth factor 1 (IGF-1) concentration or stimulated growth hormone measurements are required if growth hormone deficiency is suspected.
Specialist referral can be considered if:
- the child’s height is below the 1st percentile for age and sex according to a relevant growth chart1
- the child is significantly shorter than expected in the context of the parental heights
- growth velocity is abnormally low2 (eg below the 25th percentile for sex, with consideration of maturation level)3.
Short stature rarely requires treatment. Growth hormone can only be prescribed by a paediatrician or endocrinologist. For information about its availability on the Pharmaceutical Benefits Scheme (PBS), see Growth hormone therapy in children.