Overview of oral candidiasis and Candida-associated lesions
Candida species are a commensal organism of the oral cavity. Oral candidiasis is an opportunistic infection that is uncommon in healthy individuals; however, it occurs relatively commonly in neonates. Common risk factors for oral candidiasis lists common risk factors for oral candidiasis. Overview of oral candidiasis and Candida-associated lesions gives an overview of the clinical features, predisposing factors and management of oral candidiasis and Candida-associated lesions. If any 'red flag' features of oral mucosal disease are present, refer to an appropriate specialist.
|
Local factors |
Systemic factors |
|---|---|
|
dentures salivary gland hypofunction corticosteroid inhalers poor oral hygiene smoking |
immune compromise (eg poorly controlled diabetes) drugs (eg systemic corticosteroids, antibiotics) |
For management of oral candidiasis in patients receiving palliative care, see here.
Management of oral candidiasis in immunocompromised patients requires specialist advice.
Patients with undiagnosed HIV infection may present initially with oral candidiasis. For patients with HIV, see here for advice on systemic antifungal therapy.
|
angular cheilitis (angular stomatitis) denture-associated erythematous stomatitis (denture stomatitis) | |
|
Oral candidiasis | |
|
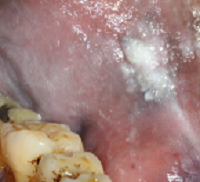
pseudomembranous candidiasis | |
|
Photo |
|
|
Clinical features |
creamy white curd, papules and plaques that are sometimes removable red, raw and often bleeding base generally asymptomatic may affect the oropharynx if the dorsal tongue is affected, autoinoculation of the palate may occur |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis neonates |
|
Management |
address predisposing factors use topical antifungal therapy for oral candidiasis if the infection affects the oropharynx, refer for specialist management |
|
erythematous candidiasis | |
|
Photo |
|
|
Clinical features |
sensitive red lesions commonly affecting the palate and tongue the tongue may appear depapillated and smooth |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis broad-spectrum antibiotic therapy |
|
Management |
address predisposing factors use topical antifungal therapy for oral candidiasis |
|
hyperplastic candidiasis | |
|
Photo |
|
|
Clinical features |
asymptomatic, nonremovable white plaques that may appear nodular usually affects the retro-commissures, anterior buccal mucosa and lateral tongue may be bilateral may resemble oral leukoplakia or oral cancer |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis |
|
Management |
address predisposing factors may be associated with epithelial dysplasia—refer to a specialist for biopsy and management [NB1] |
|
Candida-associated lesions | |
|
angular cheilitis (angular stomatitis) | |
|
Photo |
|
|
Clinical features |
painful erythema and fissuring of the corners of the mouth usually caused by a mixed infection of Candida, Staphylococcus aureus and Streptococcus species often associated with intraoral candidiasis |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis deep skin folds around the mouth (associated with worn down teeth, ill-fitting dentures or not wearing dentures) iron, folate or vitamin B12 deficiency Crohn disease granulomatous disease atopic and seborrhoeic dermatitis |
|
Management |
dental review to assess dental or denture-related causes address predisposing factors use topical antifungal therapy for angular cheilitis treat oral candidiasis, if present, with topical antifungal therapy for oral candidiasis |
|
denture-associated erythematous stomatitis (denture stomatitis) | |
|
Photo |
|
|
Clinical features |
sensitive erythematous lesions confined to denture-bearing areas, particularly the palate may appear punctate, or smooth and red nodular hyperplasia may be observed |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis ill-fitting dentures suboptimal oral and denture hygiene dietary factors |
|
Management |
advise patient to optimise denture hygiene and to remove dentures at night, clean them, then store them dry overnight (see Denture hygiene) dental review to assess fit of dentures if symptoms do not resolve after 1 month of optimal oral and denture hygiene, use topical antifungal therapy for oral candidiasis applied inside the mouth and to the dentures |
|
median rhomboid glossitis | |
|
Photo |
|
|
Clinical features |
rhomboid area of depapillation and erythema in the midline of the dorsal tongue may be fissured or nodular autoinoculation of the palate may occur usually asymptomatic although it may sting or burn |
|
Predisposing factors |
see Common risk factors for oral candidiasis for risk factors for oral candidiasis |
|
Management |
address predisposing factors use topical antifungal therapy for oral candidiasis |
Note:
NB1: The treating specialist should perform the biopsy of an oral mucosal lesion. In rural or remote areas where a delay in specialist review is expected, seek expert advice on biopsy technique—a punch biopsy is not appropriate. | |