Presentation of cutaneous lupus erythematosus
Cutaneous lupus erythematosus is an autoimmune disease affecting the skin. The three main clinical variants of cutaneous lupus erythematosus areChasset, 2019Ribero, 2017:
- chronic (discoid) cutaneous lupus erythematosus
- subacute cutaneous lupus erythematosus
- acute cutaneous lupus erythematosus.
Photosensitivity is a common feature of all three forms of cutaneous lupus erythematosus. The rash most commonly occurs on the sun-exposed areas of the face, neck, scalp, upper torso and extensor upper limbs.
Prevalence of cutaneous lupus erythematosus is higher in females than in males; however, the diagnosis is often missed in males because the condition may present atypically. There may be a higher prevalence of cutaneous lupus erythematous in ethnic populations with darker skin types (eg Aboriginal and Torres Strait Islander peoples, African American, Asian and Hispanic populations)Pons-Estel, 2010Stojan, 2018Thomas, 2020.
The characteristic lesions of chronic cutaneous (discoid) lupus erythematosus are well-defined red scaly plaques with prominent follicular plugging. Chronic lesions can be hypo- or hyper-pigmented, hypertrophic, or cause atrophic scarring (including scalp alopecia). Alopecia can be profound and extensive. Prompt effective treatment is essential to minimise the risk of permanent scarring. See here for photos of chronic (discoid) cutaneous lupus erythematosus.
Subacute cutaneous lupus erythematosus can present as photosensitive papulosquamous (well-demarcated scaly plaques) or annular (ring-like) lesions. Atrophy and scarring do not occur, but significant hypo- and hyper-pigmentation can occur. See here for photos of subacute cutaneous lupus erythematosus.
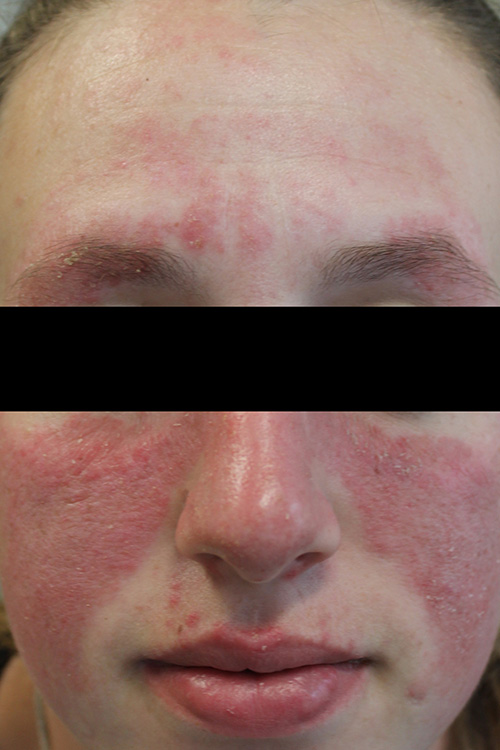
Acute cutaneous lupus erythematosus typically presents as malar erythema or a ‘butterfly rash’ (erythema and oedema over the bridge of the nose, extending onto the cheeks but sparing the nasolabial folds). This rash is usually transient and resolves without scarring, but sometimes there can be dyspigmentation.
Cutaneous lupus erythematosus can be associated with systemic lupus erythematosus. Acute cutaneous lupus erythematosus is usually associated with systemic lupus erythematosus. However, only around 50% of patients with subacute cutaneous lupus erythematosusOkon, 2013, and 5 to 10%Okon, 2013 of patients with chronic (discoid) cutaneous lupus erythematosus (especially those with a high antinuclear antibody [ANA] titre or disseminated discoid lupus lesions), fulfil the criteria for diagnosis of systemic lupus erythematosus or develop systemic lupus erythematosus during their disease course. See here for information on assessment of cutaneous lupus erythematosus, including screening for systemic lupus erythematosus.
Cutaneous lupus erythematosus can be drug-induced or drug-exacerbated in up to 20% of patients (some studies also report higher incidences)Laurinaviciene, 2017. Some commonly implicated drugs are antifungals (eg terbinafine, griseofulvin), antihypertensives (eg angiotensin converting enzyme inhibitors, beta blockers, calcium channel blockers, thiazides), statins and proton pump inhibitors.