Pityriasis rosea
Pityriasis rosea is a common, self-limiting inflammatory skin condition thought to be caused by a viral infection (reactivation of human herpesvirus 6 or 7). It mainly affects older children and young adults. The eruption begins with a herald patch that may be mistaken for tinea. About 2 weeks later, multiple scaly, oval, salmon-coloured macules appear, each about 1 to 2 cm in diameter. The macules are confined to the trunk and proximal limbs, and are arranged along the skin creases, giving the appearance of a Christmas tree. The rash may be itchy and disappears spontaneously (usually within 6 to 8 weeks). For photos of pityriasis rosea, see here.
Differential diagnoses include guttate psoriasis and secondary syphilis (see here for photos of secondary syphilis).

Reproduced with permission from the A-Z of Skin [digital]. Australasian College of Dermatologists. Sydney. https://www.dermcoll.edu.au/

Reproduced with permission from the A-Z of Skin [digital]. Australasian College of Dermatologists. Sydney. https://www.dermcoll.edu.au/

Photo sourced with permission from Professor Bart Currie.
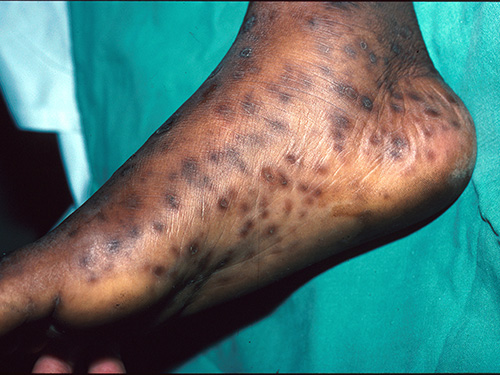
Photo sourced with permission from Professor Bart Currie.
If the patient has severe itch, apply a topical corticosteroid. Use:
1betamethasone valerate 0.02% cream topically, once or twice daily betamethasone valerate betamethasone valerate betamethasone valerate
OR
1triamcinolone acetonide 0.02% cream or ointment topically, once or twice daily. triamcinolone acetonide triamcinolone acetonide triamcinolone acetonide
Phototherapy (and cautious exposure to natural sunlight) may relieve itch and hasten resolution of the rash—refer to a dermatologist for extensive or persistent cases.