Risk assessment for medication-related osteonecrosis of the jaw
Bone-invasive dental procedures (eg tooth extractions, difficult surgical extractions, implant placement, periapical or radicular surgery, periodontal flap surgery) can trigger medication-related osteonecrosis of the jaw. However, medication-related osteonecrosis of the jaw can occur in patients who have not had a bone-invasive dental procedure, such as patients with poorly fitting dentures or exostoses (eg tori, mylohyoid ridges). Osteonecrosis that is not related to medication use can also occur at these sites spontaneously.
The risk of medication-related osteonecrosis of the jaw is higher for long durations and high doses of antiresorptive therapy, and may be higher when antiresorptive and antiangiogenic drugs are used concomitantly.
C-terminal telopeptide (CTX) is a breakdown product of bone resorption. The serum C-terminal telopeptide concentration has been proposed as a way of estimating a patient’s risk of medication-related osteonecrosis of the jaw. However, there is insufficient evidence to support a threshold serum C-terminal telopeptide concentration beyond which medication-related osteonecrosis of the jaw will not occur. Furthermore, the serum C-terminal telopeptide concentration is affected by many variables, including patient age, gender, medical conditions (eg bone disease), menopausal status, drugs (eg oral contraceptives, hormone replacement therapy, antiresorptive drugs), and the assay method used. It is therefore difficult to use a patient’s C-terminal telopeptide test result to assess the risk of medication-related osteonecrosis of the jaw.
Has the patient ever received treatment for any bone or calcium disorders or malignancy?
Antiresorptive drugs are used to treat:
- osteoporosis
- Paget disease of the bone
- cancer with spread to the bone (eg breast, prostate, liver, lung, kidney)
- multiple myeloma.
Romosozumab is used to treat osteoporosis.
Is the patient currently receiving or have they previously received treatment with an antiresorptive drug or romosozumab?
Antiresorptive drugs can be taken orally (either daily, once weekly or once monthly), or can be administered intravenously or subcutaneously and given less frequently (eg once or twice yearly). Antiresorptive drugs available in Australia are:
- alendronate
- denosumab
- ibandronic acid
- pamidronate
- risedronate
- zoledronic acid.
Romosozumab is given subcutaneously once monthly.
Has the patient received an antiangiogenic drug for the management of cancer?
Antiangiogenic drugs are used as targeted therapies for specific cancers. Some antiangiogenic drugs (cabozantinib, lenvatinib, sunitinib [tyrosine kinase inhibitors] and bevacizumab [a monoclonal antibody-targeting VEGF]) have been associated with an increased risk of medication-related osteonecrosis of the jaw; the risk may also be increased with other drugs that have a similar mechanism of action.
[NB1] [NB4]
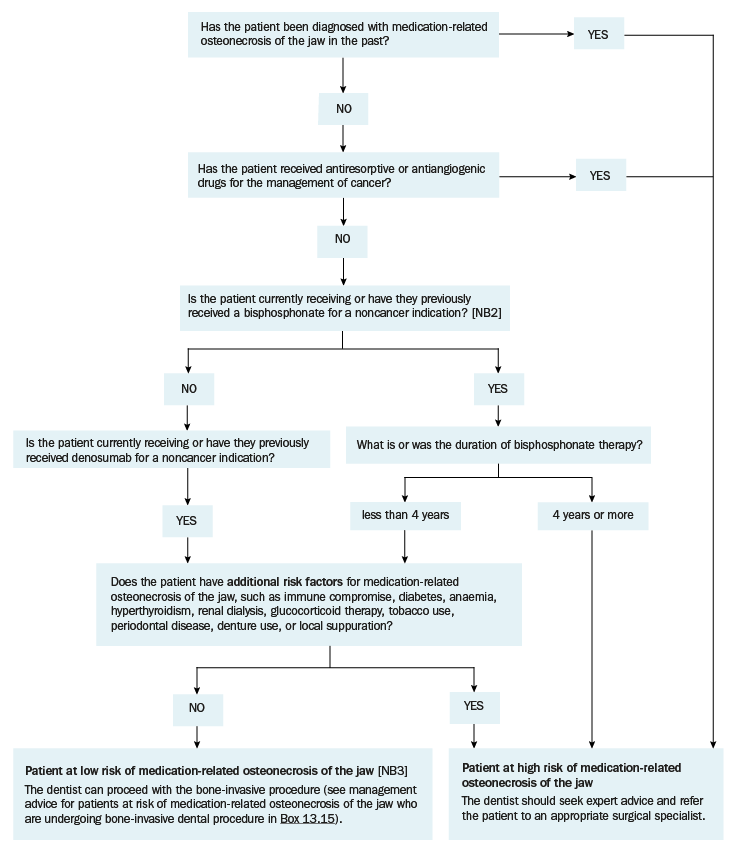
NB1: This risk assessment tool is based on limited data and cannot definitively classify a patient’s risk of medication-related osteonecrosis of the jaw.
NB2: Patients who have taken bisphosphonates in the past may still have an increased risk of medication-related osteonecrosis of the jaw because the half-life of bisphosphonates in the bone is long; it is not known how fast and to what extent the risk diminishes after stopping bisphosphonates.
NB3: Patients classified as ‘low risk’ still have a risk of medication-related osteonecrosis of the jaw that is higher than the general population.
NB4: The risk of osteonecrosis of the jaw with romosozumab is unclear so specific risk management advice has not been included. However, most patients receiving romosozumab would have had at least 12 months of therapy with an antiresorptive drug, and this should be considered when assessing the risk of medication-related osteonecrosis of the jaw.