Bleeding after oral surgery
A postoperative bleeding complication requires prompt assessment and management. Check the patient’s medical and medication history. Consider the patient’s use of drugs that can affect haemostasis (eg anticoagulants, antiplatelet drugs, complementary medicines)—see Antithrombotic drugs: considerations for oral and dental procedures for more information. Bleeding can occur when vasoconstriction induced by a local anaesthetic preparation subsides. Consider the rare possibility of a previously undiagnosed condition affecting haemostasis (eg von Willebrand disease).
For patients who have had multiple tooth extractions, if the bleeding occurs from one extraction site, it is likely to be a local cause. Conversely, if the bleeding occurs from multiple extraction sites, consider systemic causes.
If bleeding occurs after oral surgery, apply firm pressure at the surgical wound and consider using an absorbable haemostatic pack. This is sufficient to stop the bleeding in most instances, even in patients taking antiplatelet or anticoagulant therapy. Management of bleeding after oral surgery gives a suggested management protocol.
If bleeding persists despite initial management, assess the area to determine the site of the bleed (see Possible sites of persistent bleeding after tooth extraction) and perform the local haemostatic procedure (see Management of bleeding after oral surgery). Common sites of persistent bleeding after tooth extraction include the mucosa (near the floor of the mouth or the tongue) or the gingiva at the alveolar crest. Uncommon sites of persistent bleeding after tooth extraction include the side or base of the tooth socket.
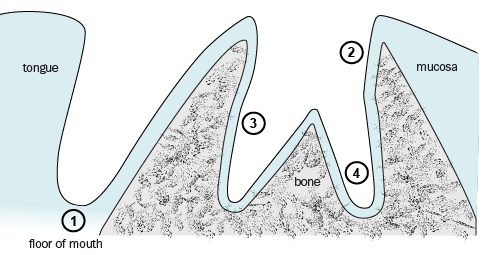
1. mucosa near the floor of the mouth—very common bleeding site
2. subgingival region—common bleeding site
3. socket wall—uncommon bleeding site
4. apical region—uncommon bleeding site
|
Initial screen and management (can be conducted by phone) |
|
Check the patient’s medical and medication history. Reassure the patient—in most cases, the following approach stops the bleeding. Advise the patient to:
Common mistakes that result in inadequate pressure at the site of bleeding include:
Advise the patient not to:
Contact the practitioner who performed the oral surgery. |
|
If bleeding does not resolve with initial management |
|
Use suction and a good light to examine the patient’s mouth to identify the bleeding site (see Possible sites of persistent bleeding after tooth extraction). Check for active bleeding. Brisk bleeding is usually from torn soft tissues rather than the socket. Ensure adequate pressure is applied to the site of bleeding. |
|
Local haemostatic procedure after applying appropriate pressure at the surgical wound |
|
Infiltrate the bleeding site with a local anaesthetic containing a vasoconstrictor. Use an absorbable haemostatic agent to pack the surgical wound. Ribbon gauze is an alternative if a haemostatic agent is not available. Tranexamic acid applied as a topical solution can be considered as an additional haemostatic method if pressure is insufficient to stop the bleeding. Tranexamic acid stabilises an existing blood clot. Either rinse the bleeding site with tranexamic acid solution or use a gauze pad soaked in tranexamic acid solution to dress the bleeding site. |
|
Emergency department transfer |
|
If the local haemostatic procedure cannot be performed or is unsuccessful in controlling the bleeding, arrange urgent transfer to an emergency department. |