Opioid dose titration in hospital
Opioids must be titrated to effect after the first dose because opioid requirements for the relief of acute pain vary up to tenfold between patients; see Moderate, acute nociceptive pain and Severe, acute nociceptive pain for initial doses. When titrating opioid doses, the adequacy of pain relief (ie the patient is comfortable, but pain is not necessarily eliminated) must be balanced against the occurrence of adverse effects.
- oral and subcutaneous opioids for moderate acute pain in adults (Example of oral and subcutaneous opioid dose titration in hospital for moderate acute pain in adults)
- oral and subcutaneous opioids for severe acute pain in adults (Example of oral and subcutaneous opioid dose titration in hospital for severe acute pain in adults)
- oral opioids for moderate or severe acute pain in children (Example of oral opioid dose titration in hospital for moderate or severe acute pain in children)
- intravenous opioids for severe acute pain in adults and children (Example of intravenous opioid dose titration in hospital for severe, acute nociceptive pain in adults and children).
For advice on tapering and stopping opioids, see here.
[NB1]
In adults, use age-based doses both initially and when titrating the opioid dose to achieve adequate pain relief and minimise adverse effects; in children, use weight-based doses [NB2].
Adhere to the requirements for safe opioid administration in hospital.
For oral, subcutaneous or intravenous administration, do not give additional opioid doses if:
- the peak effect of the dose has not yet occurred (ie approximately 1 hour after oral or subcutaneous administration, 5 minutes after intravenous administration)
- the patient has signs of opioid-induced ventilatory impairment (eg sedation score of 2 or more, reduced respiratory rate [NB3], hypoventilation, hypoxia)
- the patient has received the maximum dose that has been prescribed for the dose interval; if adequate analgesia has not been achieved, seek expert advice—the pain may not be opioid responsive, the patient may not be absorbing the opioid, or other factors may be contributing to the pain (eg psychosocial factors, undiagnosed pathology)
- pain relief is adequate (ie the patient is comfortable, but pain is not necessarily eliminated); periodic reassessment is required.
If pain relief is inadequate, oral or subcutaneous opioid doses can be titrated:
- if the dose interval has elapsed, a repeat dose may be given; the repeat dose may be smaller or larger than the previous dose(s)—its size should be informed by the amount of drug required over the previous dose interval(s) and the clinical context of the pain (eg a larger dose may be required if the patient’s pain has been exacerbated by mobilisation; a smaller dose is needed as the acute injury heals)
- if the dose interval has not elapsed and the patient has not received the maximum dose prescribed for the dose interval, a top-up dose may be given
- in general, the top-up dose should be no more than half the previous dose—it should never be larger than the dose that was administered initially
- the size of the top-up dose should be informed by the response to the previous dose (eg whether there was any relief from the previous dose; whether pain relief from the previous dose was adequate, but wore off before the dose interval elapsed)
- when the top-up dose is added to the previous doses, the total dose must not exceed the maximum prescribed dose for the interval
- the dose interval does not restart when a top-up dose is given—it is still counted from when the initial dose of the interval was administered.
For advice on tapering and stopping opioids, see here.
NB1: These principles are included to support safe use of the opioid regimens in these guidelines.
- for children who are underweight or of healthy weight, use actual body weight to calculate the dose
- for children who are overweight or obese (ie more than 20% heavier than their ideal body weight), use ideal body weight.
- children 1 to 12 years: less than 20 breaths/minute.
- children 12 to 17 years: less than 15 breaths/minute
- adults older than 17 years: less than 8 breaths/minute.
[NB1]
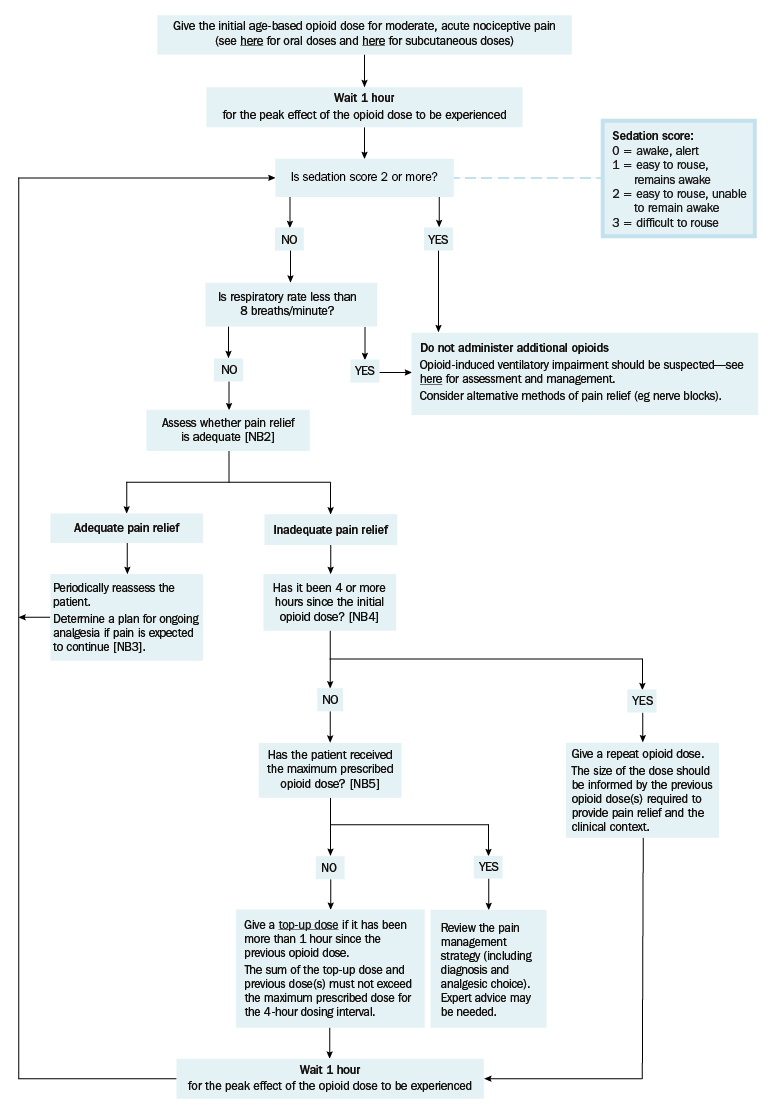
NB2: Adequate pain relief implies that the patient is comfortable; pain is not necessarily eliminated.
NB3: If the patient’s circumstances have changed (eg a dislocated shoulder has been reduced and the patient’s pain is mild), reconsider analgesic regimens.
If moderate pain is expected to continue, oral opioids should be used for ongoing analgesia. If the oral route is not suitable in adults, opioids may be administered subcutaneously via a subcutaneous cannula, or seek expert advice on the administration of opioids via patient-controlled analgesia (PCA).
NB4: The opioid dose frequency depends on the severity of pain; for moderate acute pain in hospital the opioid dose frequency is 4-hourly.
[NB1]
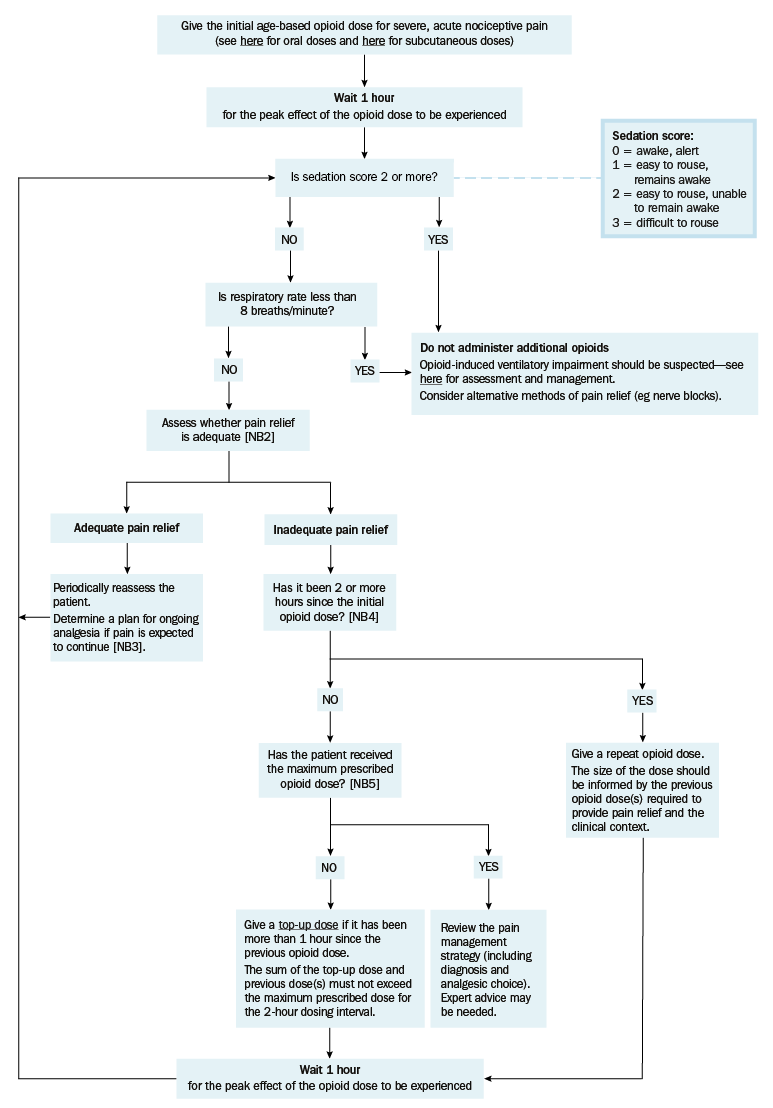
NB2: Adequate pain relief implies that the patient is comfortable; pain is not necessarily eliminated.
NB3: If the patient’s circumstances have changed (eg a dislocated shoulder has been reduced and the patient’s pain is mild), reconsider analgesic regimens.
If moderate or severe pain is expected to continue, oral opioids should be used for ongoing analgesia. If the oral route is not suitable in adults, opioids may be administered subcutaneously via a subcutaneous cannula, or seek expert advice on the administration of opioids via patient-controlled analgesia (PCA).
NB4: The opioid dose frequency depends on the severity of pain; for severe acute pain in hospital the opioid dose frequency for adults is 2-hourly.
[NB1]
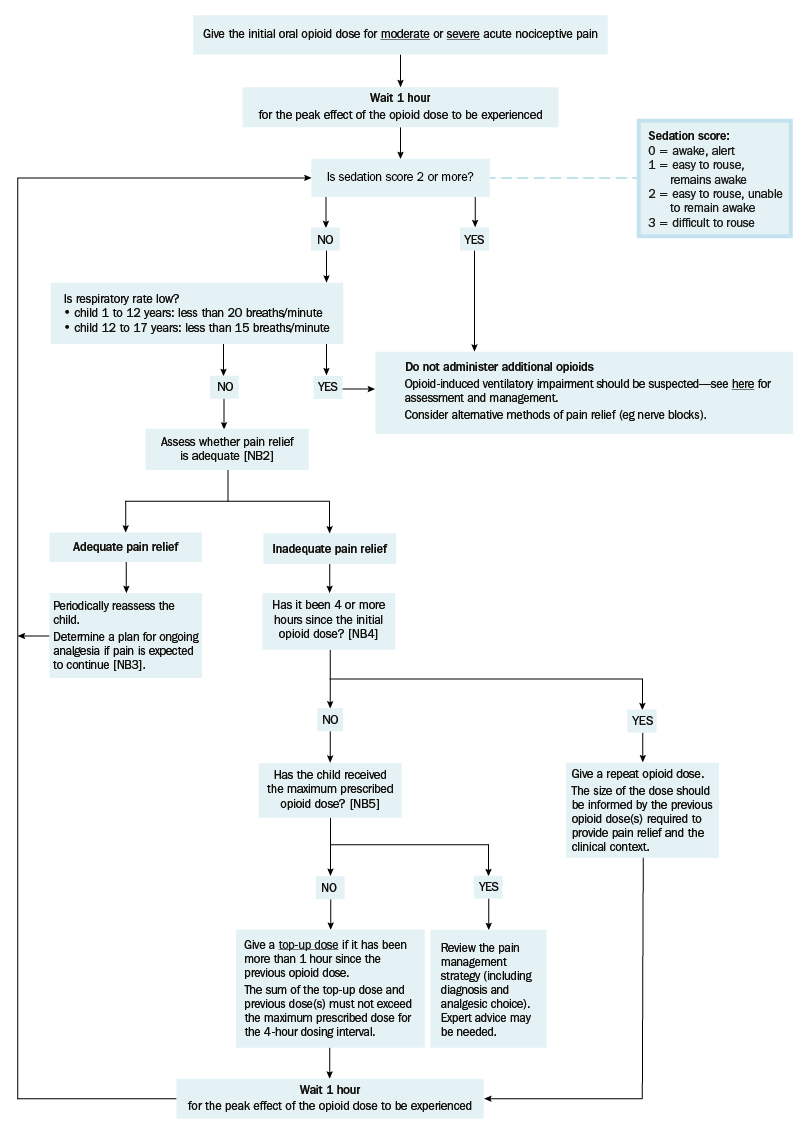
NB2: Adequate pain relief implies that the patient is comfortable; pain is not necessarily eliminated.
NB3: If the child’s circumstances have changed (eg a dislocated shoulder has been reduced and the child’s pain is mild), reconsider analgesic regimens.
NB4: The oral opioid dose frequency for children in hospital with moderate or severe acute pain is 4-hourly.
[NB1]
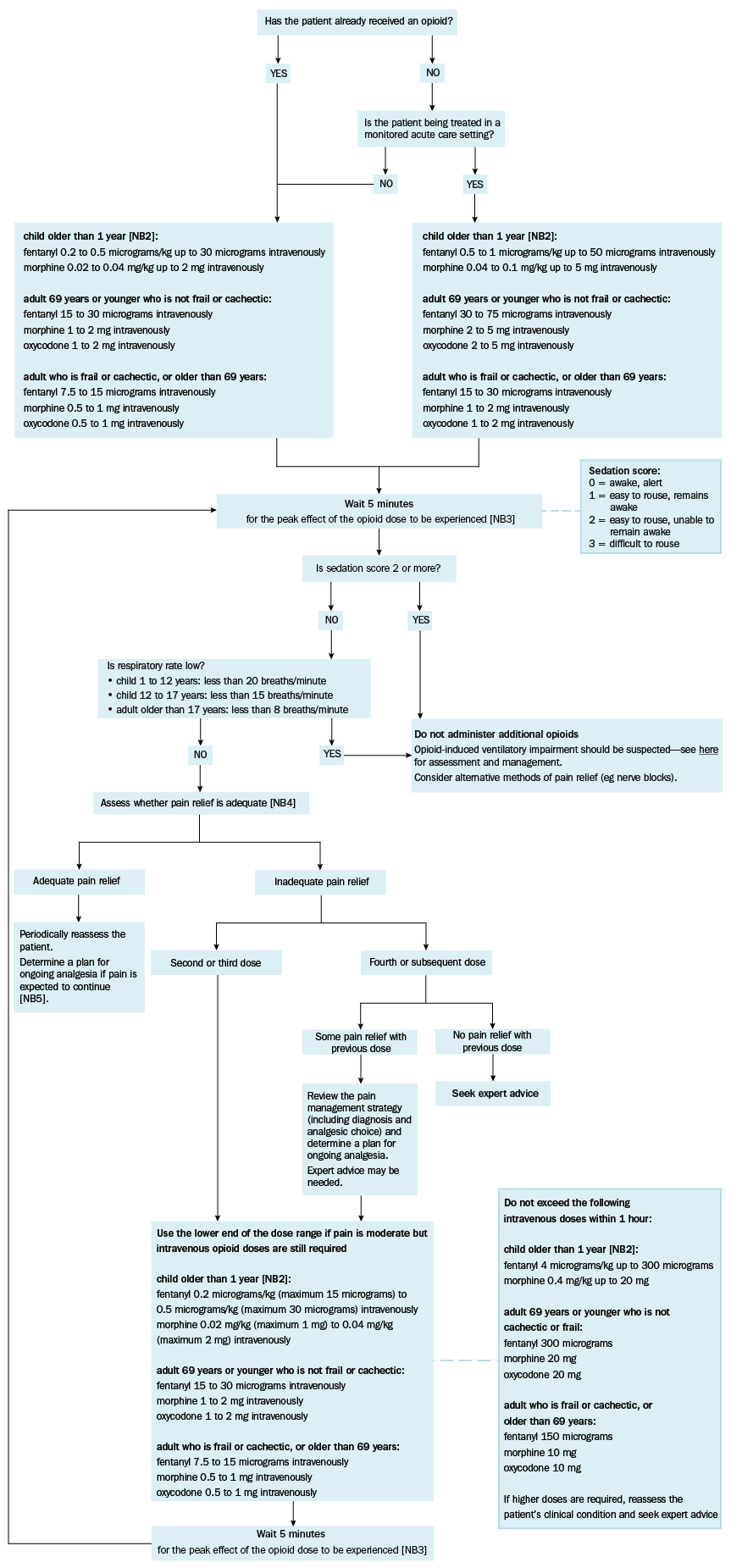
NB1: This figure is intended as an example for the initial management of severe, acute nociceptive pain in adults and children. It is not appropriate for ongoing analgesia in continuing pain. Local protocols may differ and should be followed if available.
NB2: For overweight children, use ideal body weight.
NB3: The peak effect of an intravenous dose of morphine may not occur for over 15 minutes.
NB4: Adequate pain relief implies that the patient is comfortable; pain is not necessarily eliminated.
NB5: If the patient’s circumstances have changed, reconsider analgesic regimens. If moderate or severe pain is expected to continue, oral opioids should be used for ongoing analgesia. If the oral route is not appropriate in adults, opioids may be administered subcutaneously via a subcutaneous cannula, or seek expert advice on the administration of opioids via patient-controlled analgesia (PCA). If the oral route is not appropriate in children, refer to local protocols—nurse- or patient-controlled analgesia may be considered, seek expert advice.