Causes of and investigations for secondary amenorrhoea
The most common causes of secondary amenorrhoea or oligomenorrhoea include:
- pregnancy
- perimenopause in females aged 45 years and older
- polycystic ovarian syndrome
-
hypogonadotrophic
causes, such as
- hypothalamic amenorrhoea (most commonly, functional hypothalamic amenorrhoea due to conditions such as stress, excessive exercise, systemic illness, eating disorders and very low body weight)
- pituitary tumours causing hyperprolactinaemia
- hypopituitarism (eg caused by tumours or iron storage disorders)
- hypergonadotrophic causes such as premature ovarian insufficiency and early menopause
- intrauterine adhesions; extensive scarring is known as Asherman syndrome
- medications that cause hypothalamic or pituitary suppression (eg opioids, corticosteroids, combined oral contraceptives, depot medroxyprogesterone, goserelin) or hyperprolactinaemia (eg antipsychotics, metoclopramide, domperidone, verapamil, ranitidine, selective serotonin reuptake inhibitors and tricyclic antidepressants).
Other causes of secondary amenorrhoea include other endocrine disorders (eg congenital adrenal hyperplasia, hyperthyroidism and hypothyroidism).
For investigations for causes of secondary amenorrhoea, see Investigations to determine the cause of secondary amenorrhoea.
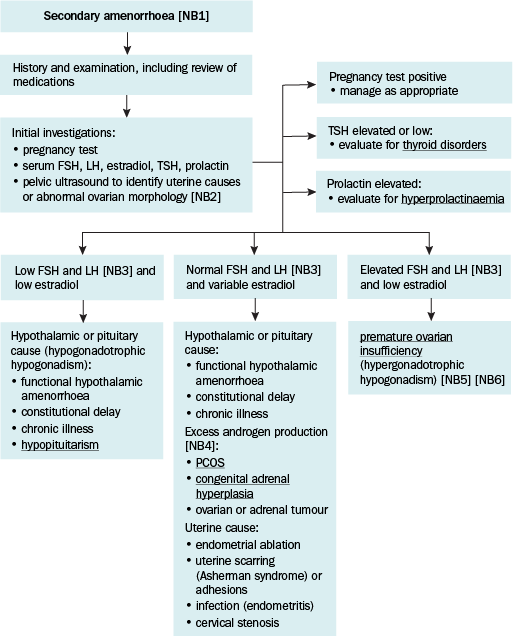
FSH = follicle stimulating hormone; LH = luteinising hormone; PCOS = polycystic ovarian syndrome, TSH = thyroid stimulating hormone
NB1: Secondary amenorrhoea is defined as the absence of menstruation for: more than 3 months in females with previously regular menstrual cycles; more than 6 months in females with previously irregular menstrual cycles.
NB2: A transvaginal ultrasound gives best detail, particularly if assessing follicle counts in premature ovarian insufficiency or in suspected PCOS. A transabdominal ultrasound is an alternative if transvaginal is not available is or is declined.
NB3: Tests may need to be repeated after 4 to 6 weeks to clarify or confirm diagnosis.
NB4: Tests for excess androgen production for conditions such as PCOS and congenital adrenal hyperplasia are appropriate if hyperandrogenism is suspected.
NB5: Ultrasound may show structural abnormalities of the ovaries in females with PCOS or ovarian tumours or some causes of premature ovarian insufficiency.
NB6: Premature ovarian insufficiency has a range of causes, including Turner syndrome.