Clinical presentation
Overview
Patients with carbamazepine poisoning can exhibit delayed onset of effects, delayed peak effects (more than 48 hours after ingestion), cyclical toxicity and coma.
Effects of carbamazepine poisoning include:
- CNS effects
- horizontal, then vertical, nystagmus
- ataxia increasing with severity, dysarthria
- agitation, fluctuating delirium
- CNS depression (altered conscious state ranging from drowsiness to coma)
- respiratory depression
- seizures
- gastrointestinal effects
- vomiting
- intermittent ileus (see Mechanism of carbamazepine-associated intermittent ileus for the mechanism of carbamazepine-associated intermittent ileus)
- pharmacobezoar formation (a mass in the gastrointestinal tract) after large ingestions of modified-release preparations; can cause altered pharmacokinetics
- cardiovascular effects
- tachycardia
- hypotension due to peripheral vasodilation and dehydration
- life-threatening arrhythmias—heart block, QRS widening and sodium channel blockade (uncommon with serum carbamazepine concentrations less than 40 mg/L [170 micromol/L]), ventricular fibrillation.
Oxcarbazepine poisoning generally causes minimal toxicity, even after massive ingestions. Effects include sedation and nausea, but more significant toxicity is rare.
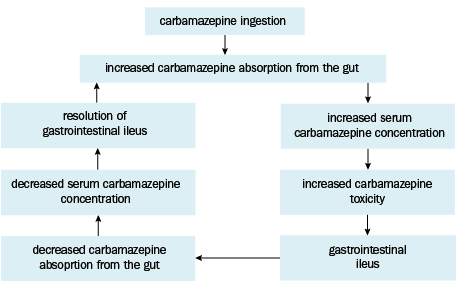
Carbamazepine-associated intermittent ileus
In carbamazepine poisoning, an increased serum carbamazepine concentration can cause gastrointestinal ileus, with temporary reduction in drug absorption from the gut lumen. As the serum drug concentration falls and ileus resolves, gut motility returns and drug absorption resumes, potentially resulting in cyclical and erratic absorption over a prolonged period, and fluctuating toxic effects. For a diagrammatic representation of this process, see Mechanism of carbamazepine-associated intermittent ileus.