Dressings for skin tears
Appropriate dressings for skin tears are described in #lwg2-c04-s4-2__tlwg2-c04-tbl2. The dressing must not cause further trauma to the wound on either application or removal, and should provide a moist wound environment, manage exudate and minimise pain. The most common approach is to use a silicone-based dressing. A small amount of an amorphous hydrogel dressing can be added to the wound bed if the wound area is at risk of drying out.
Avoid:
- alginate dressings as primary dressings on bleeding wounds—these can adhere to the wound
- skin closure strips (eg Steri-Strips, tapes)—because of the risk of damage on removal
- suturing or stapling—because the skin tissue is too fragile.
Use a cohesive or tubular retention bandage to retain dressings. Cyanoacrylate skin glue (eg Leukosan, Dermabond, Marathon) is an option for ISTAP type 1 and 2 skin tears, but require skill and knowledge to use appropriately.
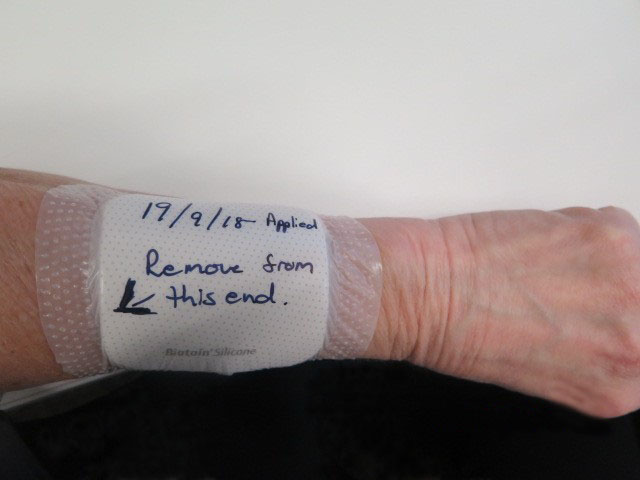
After applying an appropriate dressing, using a felt-tip pen, mark the dressing with:
- the date of application
- an indication of how to remove the dressing to avoid disturbing the skin flap, if present; see How to mark a dressing for a skin tear.
Review the dressing after 24 hours to assess exudate management—look for exudate strikethrough on the back and edges of the dressing. If a skin flap is present, aim to leave the dressing in place for at least 5 days so the flap can reconnect. Silicone mesh dressings can be left in place for 2 weeks.