Overview of drug therapy for tobacco smoking and nicotine dependence
Most people require drug therapy to make lasting changes to tobacco use, but those who have ‘low nicotine dependence’ may prefer to try behavioural intervention alone before considering adding drug therapyBaker, 2007. People are considered to have low dependence if they use tobacco more than 60 minutes after waking, particularly if they do so only in cue-driven situations (eg when out with friends in a bar).
Options for drug therapy in managing tobacco smoking and nicotine dependence are outlined in Overview of drug therapy to manage tobacco use and nicotine dependence. First-line options are:
- combination nicotine replacement therapy (NRT) (use of a slow-acting NRT [nicotine patch] with a medium-acting form [eg gum, lozenge or inhalator] and/or a fast-acting form [nicotine mist spray])
- varenicline
- bupropion.
Medium- or fast-acting NRT can be safely added to varenicline or bupropion if required to control cue-driven cravingsThe Royal Australian College of General Practitioners (RACGP), 2021Hughes, 2014. Data is lacking on combining bupropion with varenicline.
For a discussion of how to choose a therapy, see Factors affecting choice of drug therapy in tobacco smoking and nicotine dependence.
If one first-line drug therapy is not suitable or effective after an adequate trial, consider another first-line drug before considering nortriptyline or nicotine vaping products.
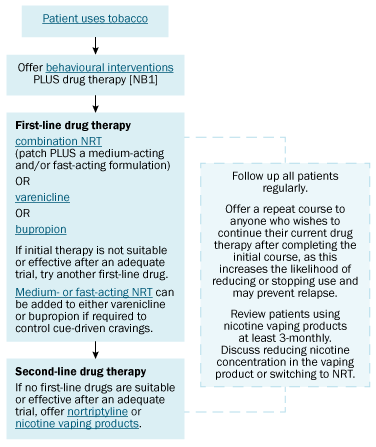
NRT = nicotine replacement therapy
NB1: People who smoke later than 60 minutes after waking are regarded as having low nicotine dependence; they may choose to try behavioural interventions alone first, especially if they smoke mainly in specific cue-driven situations (eg when out with friends in a bar). However, drug therapy can be offered if they want to start it together with behavioural interventions, or if behavioural interventions alone are not effective.