Management of primary spontaneous pneumothorax
Primary spontaneous pneumothorax is a pneumothorax that occurs without a precipitating external event in a patient without underlying lung disease.
For management of primary spontaneous pneumothorax in children, seek specialist advice. Information on the management of primary spontaneous pneumothorax in children is available from The Royal Children’s Hospital (Melbourne) website.
Spontaneous pneumothorax is diagnosed primarily on history and inspiratory chest X-ray; see Classification and diagnosis of pneumothorax for more information.
Primary spontaneous pneumothorax is usually not dangerous. Symptoms commonly resolve within 24 to 48 hours without specific treatment. Before treating primary spontaneous pneumothorax, exclude secondary spontaneous pneumothorax.
All primary spontaneous pneumothoraces, regardless of size, should initially be managed conservatively with analgesia, and oxygen if the patient is hypoxaemic. A large multicentre randomised controlled trial showed that conservative management was not inferior to pleural intervention with regard to radiological and symptom resolution in otherwise healthy patients. Compared to pleural intervention, conservative management reduced hospitalisation days, time off work, need for prolonged chest drainage and surgery, risk of early recurrence and adverse events1.
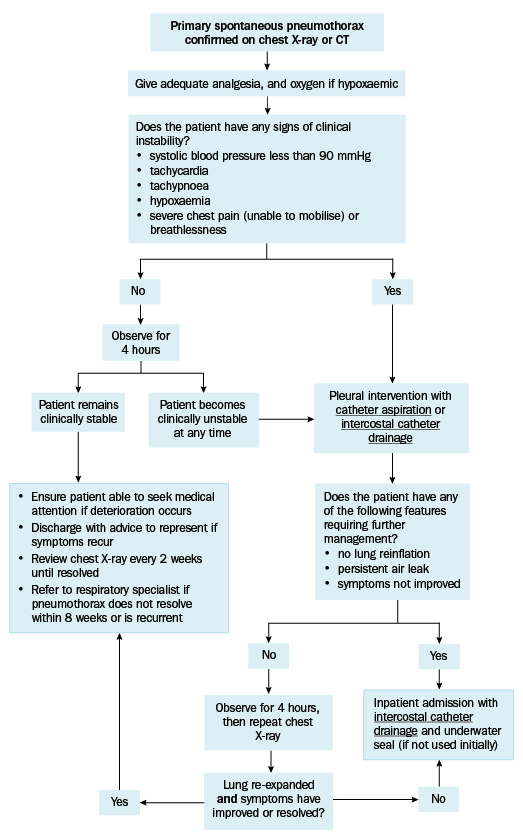
For patients with primary spontaneous pneumothorax, give adequate analgesia; this often substantially improves breathlessness, which may be largely related to the pain of breathing. For information on managing acute pain with analgesics, see Using analgesics to manage acute pain.
Give oxygen if the patient is hypoxaemic. Titrate flow of oxygen to target SpO2 levels; see here for more advice.