Principles of treatment
Mast cell activation with histamine release is the basis of all forms of urticaria, whether acute or chronic—oral antihistamines are the mainstay of therapy.
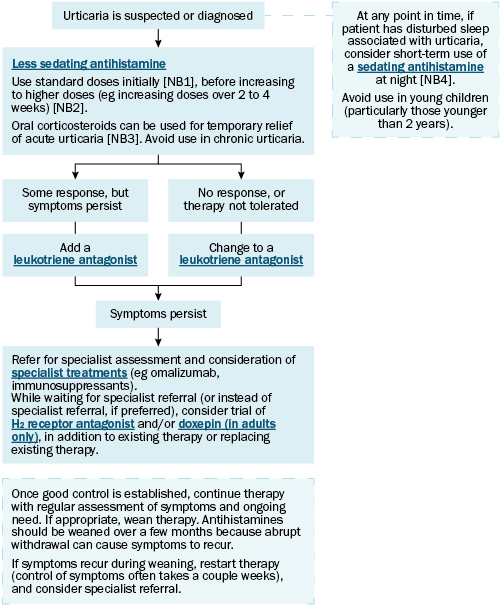
Oral corticosteroids can temporarily relieve acute urticaria, but high doses are needed, and the condition often recurs when treatment stops. Avoid oral corticosteroids for chronic urticaria.
For urticaria, trial a less-sedating antihistamine at standard doses, before increasing to higher doses (eg increasing doses over 2 to 4 weeks).
If there is no response, or the patient does not tolerate the antihistamine, change to a leukotriene antagonist (eg montelukast). However, if there is some response to the antihistamine but symptoms still persist, consider adding a leukotriene antagonist .
If symptoms still persist, consider referring to a specialist (eg dermatologist, allergist, immunologist) for omalizumab and other specialist treatments . While waiting for specialist referral (or instead of specialist referral, if preferred), consider trialling a histamine H2-receptor antagonist and/or doxepin (in adults only) (either as an addition to existing therapy, or as an alternative to existing therapy).
For adults and older children with disturbed sleep associated with urticaria, consider using a sedating antihistamine at night.
Advise patients to avoid exposure to any triggers, if possible.
Once good control is established, continue therapy with regular assessment of symptoms and ongoing treatment need. If appropriate, wean therapy. Antihistamines should be weaned over a few months because abrupt withdrawal can cause symptoms to recur. Warn patients that urticaria can recur and that they may need to restart treatment. If symptoms recur during weaning, restart therapy (control of symptoms often takes a couple of weeks), and consider specialist referral.
Approximately 50% of patients with chronic urticaria have resolution within 3 months; however, symptoms can persist for more than 12 months in 20% of patientsAustralasian society of clinical immunology and allergy (ASCIA) CSU working party, 2020.
Approximately 40% of patients with chronic urticaria also have angioedema. The presence of angioedema or thyroid antibodies is associated with more persistent disease. Urticaria with angioedema is treated as for urticaria.
NB1: Response and tolerance of a less-sedating antihistamine varies between patients. If therapy with one less-sedating antihistamine is not effective or causes drowsiness during the day, change to a different less-sedating antihistamine. Sedating potential of less-sedating antihistamines can vary between patients; of the less-sedating antihistamines, cetirizine is the most likely to cause sedation.
NB2: Up to four times the standard dose can be used in adults. In children, up to four times the standard dose of cetirizine can be used; however, if long-term therapy is required, consider specialist referral and assessment for other treatment options (eg omalizumab).
NB3: Oral corticosteroids can temporarily relieve acute urticaria, but high doses are needed and the condition often recurs when treatment stops.
NB4: Avoid long-term use of sedating antihistamines. If sedating antihistamines are being used for more than a few days, seek specialist advice or referral.