Overview of electrocardiography
In patients with a suspected poisoning, perform a 12-lead electrocardiogram (ECG) to detect QRS widening, QT-interval prolongation, arrhythmias and other ECG changes seen in:
- adrenoceptor stimulation (eg stimulant drug poisoning) or blockade (eg beta-blocker poisoning)
- calcium channel blockade (eg calcium channel blocker poisoning)
- sodium-potassium adenosine triphosphatase (ATPase) pump blockade (eg digoxin poisoning)
- toxin-mediated myocardial ischaemia (eg carbon monoxide poisoning, cocaine poisoning, cyanide poisoning, methaemoglobinaemia).
Undertake a risk assessment to determine whether to perform continuous ECG monitoring (to monitor heart rate and rhythm) and serial 12-lead ECGs (to identify evolving ECG changes and make accurate measurements).
A diagrammatic representation of a normal ECG complex is shown in Diagrammatic representation of a normal electrocardiogram (ECG) complex.
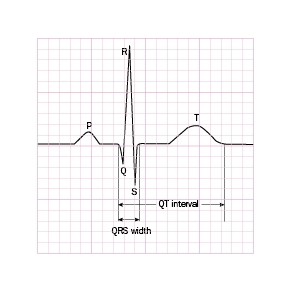
On a standard 12-lead ECG, 1 millimetre = 40 milliseconds (in this figure, 1 small square is 1 mm). The QRS width is measured from the start of the Q wave to the end of the S wave and is normally less than 120 milliseconds. The QT interval is measured from the start of the Q wave to the end of the T wave. The normal QT interval varies with heart rate and can be corrected for heart rate, but generally it is less than 440 milliseconds.