Assessment for QT-interval prolongation and torsades de pointes
Drug-induced QT-interval prolongation may be associated with torsades de pointes (polymorphic ventricular tachycardia) and, less commonly, other arrhythmias. Torsades de pointes is frequently self-limiting; however, it can be life threatening if it progresses to sustained ventricular tachycardia or ventricular fibrillation (cardiac arrest).
Drug-induced QT-interval prolongation is due to delayed cardiac repolarisation, most commonly from potassium channel blockade, but can also occur with hypokalaemia, hypocalcaemia and hypomagnesaemia. Drugs highly associated with QT-interval prolongation and torsades de pointes are listed in Drugs highly associated with QT-interval prolongation and torsades de pointes.
The QT interval may be prolonged in association with QRS widening, but this rarely causes torsades de pointes1.
|
Drug class |
Drug |
|---|---|
|
antiarrhythmics |
amiodarone disopyramide sotalol |
|
antidepressants |
citalopram, escitalopram tricyclic antidepressants [NB1] |
|
antihistamines |
dimenhydrinate, diphenhydramine loratadine |
|
antimicrobials |
ciprofloxacin clarithromycin erythromycin fluconazole moxifloxacin pentamidine voriconazole |
|
antipsychotics |
amisulpride chlorpromazine haloperidol ziprasidone |
|
chemotherapeutic agents |
arsenic |
|
other drugs |
chloroquine, hydroxychloroquine and quinine cocaine domperidone loperamide, methadone, oxycodone organophosphate and carbamate pesticides |
|
Note: NB1: QT-interval prolongation caused by tricyclic antidepressants is usually due to QRS widening and there is no true lengthening of the JT interval (defined as the QT interval minus the QRS width).
| |
Measure the QT interval manually on a 12-lead ECG, preferably in multiple leads including limb lead II. Do not rely on ECG machine–generated measurements of the QT interval and corrected QT interval (QTc). They can under-measure the QT interval by up to 200 milliseconds and falsely reassure the clinician in the presence of extreme QT-interval prolongation in poisoning. In patients with tachycardia, the automated calculations of QTc interval may be incorrect due to an error of measurement or overcorrection for the heart rate.
Use the QT-interval nomogram in QT-interval nomogram to assess risk of drug-induced torsades de pointes to assess for genuine QT-interval prolongation in poisonings; when the measured QT interval and heart rate (QT interval/heart rate pair) plots above the nomogram line, the QT interval is prolonged and the patient is at risk of developing torsades de pointes. In patients with QT-interval prolongation, the magnitude of risk for developing torsades de pointes is greater at slower heart rates.
Genuine QT-interval prolongation requires continuous ECG monitoring and serial 12-lead ECGs. For treatment of QT-interval prolongation due to poisoning, see here.
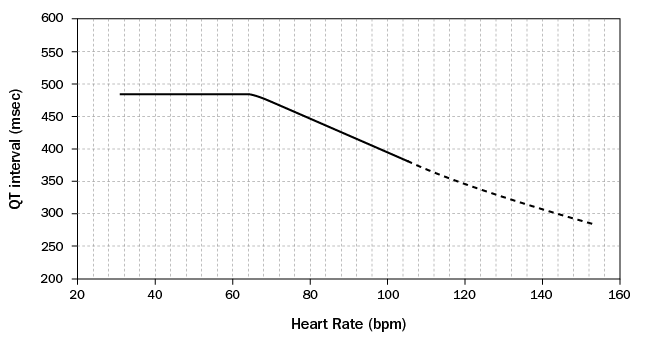
Measure the QT interval manually on a 12-lead ECG from the beginning of the Q wave to the end of the T wave in multiple leads (six leads including limb and chest leads), and calculate the median QT interval (see Diagrammatic representation of a normal electrocardiogram (ECG) complex for a diagrammatic representation of a normal ECG complex). On the nomogram, plot the median QT interval versus the heart rate recorded on the ECG (QT interval/heart rate pair). If the point is above the nomogram line, the patient is at risk of developing torsades de pointes.
Reproduced with permission of Oxford University Press from Chan A, Isbister GK, Kirkpatrick CM, Dufful SB. Drug-induced QT prolongation and torsades de pointes: evaluation of a QT nomogram. QJM 2007; 100(10):609-15. [URL]