Indications for acetylcysteine therapy
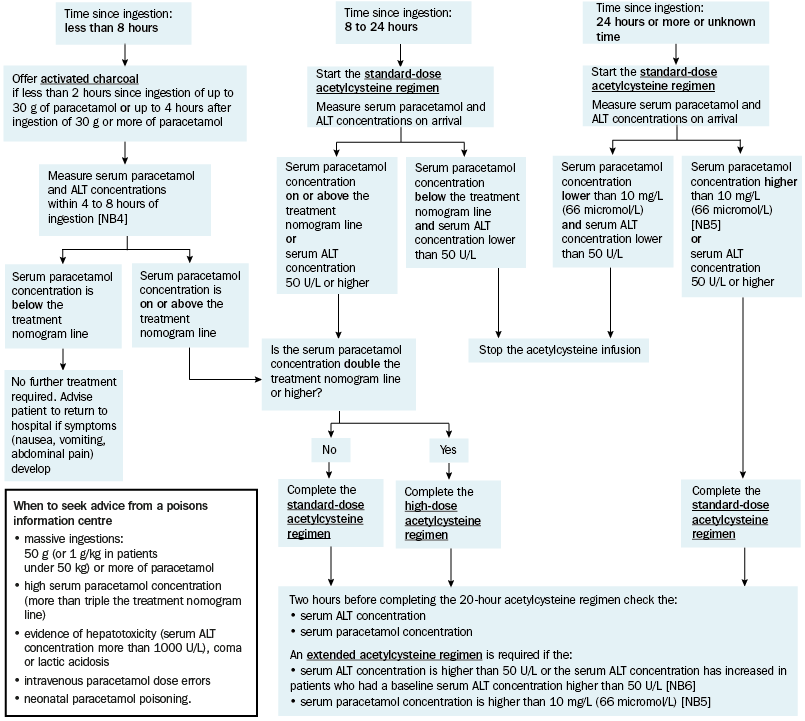
The use of acetylcysteine for immediate-release paracetamol poisoning depends on the:
- serum paracetamol concentration
- time since ingestion
- serum alanine aminotransferase (ALT) concentration in those presenting more than 8 hours after ingestion.
The risk of acute liver injury increases if there is a delay of more than 8 hours to acetylcysteine treatment after an acute ingestion of immediate-release paracetamol. If the serum paracetamol concentration will not be available within 8 hours, start acetylcysteine therapy immediately, without using the nomogram.
Some patients require an extended acetylcysteine regimen beyond the 20-hour regimen because they are at greater risk of developing acute liver injury. To determine the need for an extended acetylcysteine regimen, measure the serum ALT and paracetamol concentrations 2 hours before completion of the 20-hour acetylcysteine regimen in all patients.
An extended acetylcysteine regimen is warranted if the:
- serum ALT concentration is higher than 50 U/L or serum ALT concentration has increased in patients who had a baseline serum ALT concentration of 50 U/L or higher (eg in patients with pre-existing liver biochemistry abnormalities)2
- serum paracetamol concentration is higher than 10 mg/L (66 micromol/L)3.
|
Time from ingestion of immediate-release paracetamol to obtaining serum paracetamol concentration result |
Action |
|---|---|
|
serum paracetamol concentration is available within 4 to 8 hours of ingestion |
If the serum paracetamol concentration is below the treatment nomogram line, acetylcysteine therapy is not indicated. If the serum paracetamol concentration is on or above (but less than double) the treatment nomogram line, complete the standard-dose acetylcysteine regimen. If the serum paracetamol concentration is double the treatment nomogram line or higher, complete the high-dose acetylcysteine regimen. |
|
paracetamol ingested 8 to 24 hours before presentation |
Start the standard-dose acetylcysteine regimen—do not wait for the serum paracetamol or ALT concentration results. When the results are available: If the serum paracetamol concentration is below the treatment nomogram line and the serum ALT concentration is lower than 50 U/L, stop the infusion. If the serum paracetamol concentration is on or above (but less than double) the treatment nomogram line or the serum ALT concentration is 50 U/L or higher, complete the standard-dose acetylcysteine regimen. If the serum paracetamol concentration is double the treatment nomogram line or higher, complete the high-dose acetylcysteine regimen. |
|
paracetamol ingested more than 24 hours before presentation or unknown time since ingestion |
Start the standard-dose acetylcysteine regimen—do not wait for the serum paracetamol concentration or ALT concentration results. When the results are available: If the serum paracetamol concentration is lower than 10 mg/L (66 micromol/L) and the serum ALT concentration is lower than 50 U/L, stop the infusion. If the serum paracetamol concentration is higher than 10 mg/L (66 micromol/L) or the serum ALT concentration is 50 U/L or higher, complete the standard-dose acetylcysteine regimen. If the serum paracetamol concentration is 100 mg/L (660 micromol/L) or higher, seek advice from a clinical toxicologist. |
Note: NB1: Seek advice from a poisons information centre for:
| |
|
Time from ingestion of immediate-release paracetamol to obtaining serum paracetamol concentration result |
Action |
|---|---|
|
serum paracetamol concentration is available within 4 to 8 hours of first ingestion [NB2] |
If the serum paracetamol concentration is on or above (but less than double) the treatment nomogram line, complete the standard-dose acetylcysteine regimen. If the serum paracetamol concentration is double the treatment nomogram line or higher, complete the high-dose acetylcysteine regimen. If the serum paracetamol concentration is below the treatment nomogram line and paracetamol was not ingested within 2 hours of blood being taken, acetylcysteine therapy is not indicated. If the serum paracetamol concentration is below the treatment nomogram line but paracetamol was ingested within 2 hours of blood being taken, measure the serum paracetamol concentration again 2 hours later. If the second serum paracetamol concentration is on or above the treatment nomogram line, complete the standard-dose acetylcysteine regimen. If the second serum paracetamol concentration is below the treatment nomogram line, acetylcysteine therapy is not indicated. |
|
serum paracetamol concentration is not available within 8 hours of first ingestion [NB2] or unknown time since first ingestion |
Start the standard-dose acetylcysteine regimen—do not wait for the serum paracetamol or ALT concentrations. When the results are available: If the first serum paracetamol concentration is below the treatment nomogram line and the first serum ALT concentration is lower than 50 U/L and paracetamol was not ingested within 2 hours of blood being taken, stop the infusion. If the first serum paracetamol concentration is below the treatment nomogram line, but paracetamol was ingested within 2 hours of blood being taken, measure the serum paracetamol and ALT concentrations again 2 hours later. If the second serum paracetamol concentration is on or above (but less than double) the treatment nomogram line or the second serum ALT concentration is 50 U/L or higher, complete the standard-dose acetylcysteine regimen. If either the first or second serum paracetamol concentration is double the treatment nomogram line or higher, complete the high-dose acetylcysteine regimen. If the second serum paracetamol concentration is below the treatment nomogram line, stop the infusion. |
|
Note:
NB1: Seek advice from a poisons information centre for:
NB2: If the patient has taken multiple staggered doses, plot the time of the first dose on the nomogram. | |
[NB1] [NB2] [NB3]
ALT = alanine aminotransferase
NB2: If the patient is a child younger than 6 years who has ingested liquid paracetamol, see Paracetamol poisoning: liquid formulations in a child younger than 6 years.
NB3: If the patient has taken a mixture of immediate-release and modified-release paracetamol tablets, treat as for modified-release paracetamol poisoning.
NB4: If the serum paracetamol concentration is not available within 8 hours of ingestion, treat as for ‘Time since ingestion: 8 to 24 hours’.
NB5: If the serum paracetamol concentration is higher than 100 mg/L (660 micromol/L), seek advice from a clinical toxicologist.
NB6: Patients with significant acute liver injury have a high or rapidly rising serum ALT concentration. Small fluctuations in ALT (eg 20 U/L or 10%) are common and do not on their own indicate the need for ongoing acetylcysteine therapy.